What Is Carpal Tunnel Syndrome?
Carpal tunnel syndrome is one of a group of disorders categorized by several different terms: repetitive stress injuries, cumulative trauma disorder, overuse syndromes, chronic upper limb pain syndrome, or repetitive motion disorders. All of these problems are generally associated with repetitive and forceful use of the hands that damage muscles and bones of the upper extremities.
 Usually, carpal tunnel syndrome (CTS) is considered an inflammatory disorder caused by repetitive stress, physical injury, or other conditions that cause the tissues around the median nerve to become swollen. It occurs either when the protective lining of the tendons within the carpal tunnel become inflamed and swell or when the ligament that forms the roof becomes thicker and broader.
Usually, carpal tunnel syndrome (CTS) is considered an inflammatory disorder caused by repetitive stress, physical injury, or other conditions that cause the tissues around the median nerve to become swollen. It occurs either when the protective lining of the tendons within the carpal tunnel become inflamed and swell or when the ligament that forms the roof becomes thicker and broader.
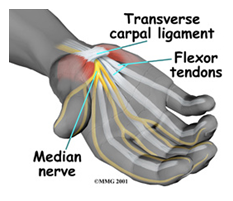
The carpal tunnel is a passageway that runs from the forearm through the wrist. Bones form three walls of the tunnel and a strong, broad ligament bridges over them. The median nerve, which supplies feeling to the thumb, index, and ring fingers, and the nine tendons that flex the fingers, passes through this tunnel. This nerve also provides function for the muscles at the base of the thumb (the thenar muscles). 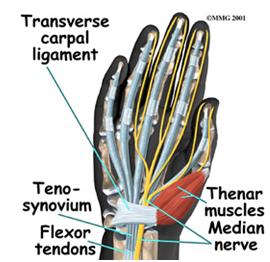
Just as stepping on a hose slows the flow of water through a garden hose, so does compression on the median nerve fibers by the swollen tendons and thickened ligament slows down the transmission of nerve signals through the carpal tunnel. The result is pain, numbness, and tingling in the wrist, hand, and fingers in the median nerve distribution of the hand, typically the thumb, index, long and ring fingers.
The longer the median nerve is compressed the more permanent can be the damage to the nerve fibers. Therefore, earlier the treatment to relieve pressure on the nerve the better the prognosis.
Carpal tunnel syndrome occurs when the median nerve, which runs from the forearm into the hand, becomes pressed or squeezed at the wrist. The median nerve controls sensations to the palm side of the thumb and fingers (although not the little finger), as well as impulses to some small muscles in the hand that allow the fingers and thumb to move. The carpal tunnel – a narrow, rigid passageway of ligament and bones at the base of the hand – houses the median nerve and tendons. Sometimes, thickening from irritated tendons or other swelling narrows the tunnel and causes the median nerve to be compressed. The result may be pain, weakness, or numbness in the hand and wrist, radiating up the arm. Although painful sensations may indicate other conditions, carpal tunnel syndrome is the most common and widely known of the entrapment neuropathies in which the body’s peripheral nerves are compressed or traumatized.
Reference: National Institute of Health